SHG linked Primary Health Care using AI
Case Study Scenario:
South Asia is currently undergoing an epidemiological transition with significantly increasing prevalence rates of both communicable and non-communicable diseases (NCDs). India is the most significant contributor to the NCD burden.
Several studies conducted over the last two decades have highlighted the high overall burden of diabetes, hypertension and dyslipidaemia in India.
According to Lancet estimates, 11.4% of the Indian population was living with diabetes in 2023, and 15.3% were prediabetic.
An example case design that will be sketched for the proof of concept is that for diabetes.
Evidence shows that patient-centred PHC, in line with a chronic care model, ensures optimal diabetes self-management support and improves long-term clinical and health outcomes in diabetes patients. While public PHC in India provides free services to patients, it lacks patient-centred care. This undermines diabetes self-management education and support.
In addition, factors such as patients' lack of knowledge about diabetes, suboptimal medication adherence, persistent clinical inertia and lack of data for monitoring and evaluation through clinical trials deteriorate the standards of diabetes care in India's PHC. Establishing guidelines, supporting health care professionals´ knowledge and skills in prediabetes and diabetes care, and implementing interprofessional referral pathways can enhance prediabetes detection and care precedence in primary health care. Deep learning models can support healthcare professionals with these tasks.
Background & Purpose:
In 2021, over half of the global population lacked full access to essential health services. This highlights the importance of achieving universal health coverage (UHC), i.e. that all people have access to the full range of quality health services they need, when and where they need them, without financial hardship, by 2030. Limited financial resources for healthcare due to various ongoing crises make it crucial to implement strategic approaches and strengthen health systems, with primary healthcare (PHC) playing a significant role. PHC enables health systems to support a person’s health needs throughout their life course – from health promotion to disease prevention, treatment, rehabilitation, palliative care and more. PHC is considered the most inclusive and cost-effective method for achieving UHC, enabling significant cost efficiencies and enhancing the resilience of health systems. Digital approaches further improve access to care by reducing costs and providing real-time healthcare delivery, especially in low-resource settings.
Self-help groups (SHGs) have emerged as powerful tools for poverty alleviation and empowerment in low- and middle-income economies. These voluntary associations bring together economically disadvantaged individuals from similar socio-economic backgrounds with the aim towards addressing common issues through self-help initiatives and community action. By pooling resources through collective action, SHGs can alleviate financial constraints and make healthcare services more affordable. At the same time, they engage in educational programmes that disseminate important information about preventative measures to promote healthy habits in their communities.
As technology becomes increasingly accessible, integrating AI tools into SHG programs emerges as the next evolutionary step. The integration of AI into SHG programs holds immense potential to revolutionise how these groups operate and deliver services, ultimately leading to improved health outcomes and empowerment of their members.
This project aims to understand and deploy a pioneering AI digital public service to enhance access to PHC for members of SHGs and their families, with a particular focus on low-resource settings.
The research project aims to understand how AI can reduce barriers such as limited healthcare infrastructure, geographical constraints, and socioeconomic factors often hindering access to essential health services. By understanding the unique challenges faced by SHG members and their families as well as the opportunities, the project seeks to identify AI-driven solutions tailored to their needs, including telemedicine platforms, mobile health applications, and community health worker support systems. Through research and experimentation, the project aims to demonstrate the feasibility and effectiveness of AI in enhancing PHC access and improving health outcomes for underserved populations in low-income settings.
Artificial Intelligence, or AI, is increasingly recognised as having significant importance to the provision of PHC. AI can enable remote consultations through telemedicine platforms, offer personalised health advice via chatbots and virtual assistants, aid in early diagnosis through symptom analysis, analyse healthcare data for resource allocation, and enhance capacity building through educational tools and training programs. These AI-driven solutions help overcome geographical barriers, empower individuals to manage their health effectively, and optimise healthcare delivery to meet the needs of underserved communities.
Sentient Bot AI Healthcare Use Case
Beneficiary Workflow:
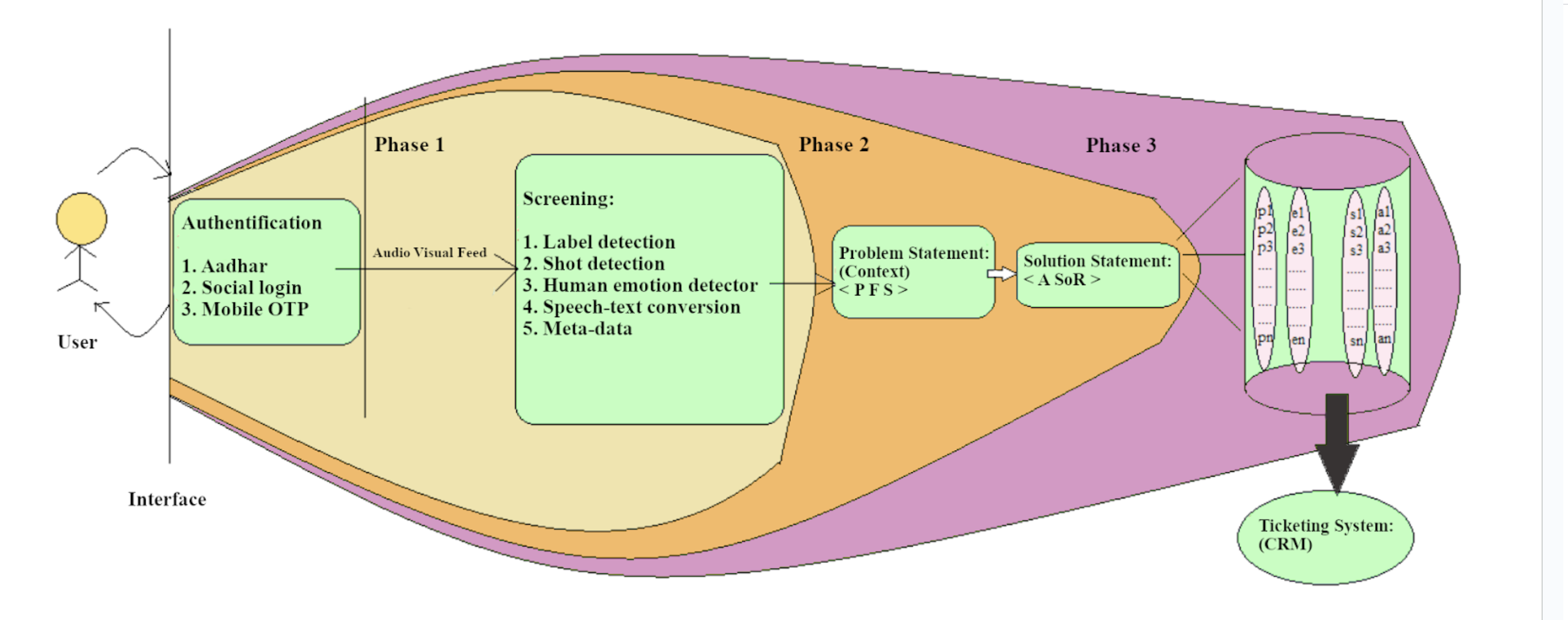
Phase 1: After self-identification, a patient beneficiary can input their video stream to the service through any smartphone chat app like WhatsApp or Telegram.
The Sentient Bot AI service screens the audio/video streams for spam and filters for label and shot detection. During this advanced screening, human sentiment combined with patient symptoms is analysed and classified using the embedded knowledge base of the AI.
Phase 2: The ‘Patient Case Summary’ is logged in the distributed database as a Problem Statement (Context). This is mapped to an inferred diagnosis, and Sentient Bot tells the patient beneficiary the inferred diagnosis along with attached notes.
The attached notes contain:
Information about the disease focused on disease progression, incubation and recovery
The localised data set about the disease
Possible treatment plans - self-administered, symptom observation schedules
A course of Action to receive treatment from healthcare providers
Affiliated health care insurance of the patient, government subsidy on the treatment plans
Phase 3: The Patient Case Summary then awaits a human review so that the patient beneficiary can receive or self-administer treatment related to the diagnosis.
The human review is conducted by an approved and registered health worker. This member accesses the processor side of the Sentient Bot AI service.
When the health worker reviews the inferred diagnosis, the Patient Case Summary is logged into the beneficiary relationship management database. This database is available for stakeholder systems integration (an organisation where a health care worker is affiliated, e.g. Hospitals, Clinics, Non-profit organisations), and public health care systems using secure API (Application programming interface) standards.
Health workers act on different levels of the embedded knowledge base:
When reviewing any inferred diagnosis
Changing the state of the ticket logged with the Patient Case Summary
Patient Case Summary is added to the larger pool of the database to fine-tune the core diagnosis model.
Specific use cases of health promotion, disease prevention, treatment, and rehabilitation in primary healthcare encompass a diverse range of applications. Through our research, we aim to develop default sets of data models tailored to address these needs effectively. These models are intended to support self-administered treatment and optimize treatment routing for communicable diseases to track and prevent their spread. Additionally, they will facilitate treatment routing for non-communicable diseases, with a particular focus on cardiometabolic diseases, where rehabilitation and recovery necessitate continuous monitoring of health data throughout the recovery period.
Following default data models are involved in the project activity:
Diagnosis Inference Model for a collection of data on local disease burden - the ability to generate a diagnosis inference without human intervention, and human intervention is only required for treatment routing approval.
Treatment Routing and Self-Administration Model - the ability to tell when self-administered treatment is enough or when routing to a nearby healthcare facility is needed.
Following default data models are involved in the project activity:
Diagnosis Inference Model for a collection of localized diseases - the ability to generate a diagnosis inference without human intervention, and human intervention is only required for treatment routing approval.
Treatment Routing and Self Administeration Model - the ability to tell when self-treatment is enough or when routing to a nearby healthcare facility is needed.
Technology Resources Used:
The following technology projects are used in this project of the Global Health Program.
Project of Muellners Foundation | Github Repository: | License | Usage |
Sentient Bot AI tool | OCL v1 | (1) Conversational Agent over voice, text and video | |
Finscale AI | OCl v1 | (1) Beneficiary Identity (2)Accounting of provisioning of health care services |
Summary of Technology Development:(Current Progress)
AI Subnet processors are available to any healthcare provider to access beneficiary healthcare records and identity to provide adequate and appropriate health care to the beneficiary. The processors can be used to do the following in real time while administering health care to the beneficiary:
(1) identify a beneficiary patient,
(2) access a beneficiary’s health record,
(3) access the region’s infection and disease prevention data sets and map the intelligence to the case records of the beneficiary,
(4) access the beneficiary’s insurance records and applicability to the disease prevention scenario,
(5) audio/video stream and understand patient sentiment, extract information from a localised knowledge base to administer health care,
(6) improve the localised knowledge base to train the machine intelligence; the improved knowledge base can also be used to train health care professionals for disease prevention.
Healthcare professionals can use the AI service - Sentient Bot as an assistant app (voice, chat or audio) to access the records. Instead of using a self-service application with a stricter use case flow, healthcare professionals can just speak into their mobile phones and interface with the knowledge base and records for the above use cases.
About Computing Infrastructure:
The underlying computing and data residency infrastructure for the embedded knowledge base of the processors that power this healthcare AI service has been deployed and is generally accessible through public APIs(Application Programming Interface).
The ticketing system is generally accessible as a Help Portal, where case requests are logged.
Additional beneficiary data is encrypted and stored on the devices of the beneficiary, and the model’s training data sets are stored on a distributed cloud computing infrastructure and
Status of Project:
Key Status Milestone in setting up project infrastructure and project cohort:
The platform subnet is designed to be HIPAA compliant(attach URL of the contract with Atlassian, Google Cloud and AWS)
Tracks the carbon footprint of the platform itself.
https://govern.muellnersfoundation.org/open-bank-protocols/carbon
The Sentient Bot AI document, speech-to-text, and sentiment processor endpoints are now available for integration into Health Care Systems.
The Bot's conversation model has been specifically designed to engage with beneficiaries using Governance Articles.
Beneficiaries can access the Bot through Telegram and Google chat platforms.
Thanks to ongoing support from the Muellners Foundation, the beneficiary identity data model is fully prepared.
This research project further aims to develop the two remaining data models essential for commercializing the digital public service:
Inferred diagnosis model
Treatment Routing model for any registered healthcare organization/clinic
The embedded knowledge base, which includes data sets and repositories feeding into the bot service as depicted in the diagram above, has been deployed for healthcare practitioners to refine using textual input.
Methods and Design:
Description of the individual activities and how these are incorporated into an overall plan related to the purpose of the project.
Methods:
Literature Review: Conduct a comprehensive review of existing literature on AI applications in healthcare, specifically focusing on primary healthcare delivery and its implications for low-income settings. This review also encompasses studies examining the role of SHGs in healthcare access and outcomes.
Needs Assessment: Perform a needs assessment within SHGs and their communities to identify specific healthcare challenges, preferences, and barriers to access. This may involve surveys, interviews, focus group discussions, and observations to gather insights from SHG members, community leaders, healthcare providers, and other stakeholders.
Technology Assessment: Evaluate the suitability and feasibility of different AI technologies for addressing the identified healthcare needs and challenges. This assessment should consider factors such as affordability, accessibility, usability, scalability, and cultural appropriateness within the context of low-income settings and SHG dynamics.
Pilot Implementation: Implement pilot interventions using selected AI technologies to enhance access to PHC within SHGs and their communities. This may involve deploying telemedicine platforms, mobile health applications, or AI-driven decision support systems, depending on the identified needs and priorities.
Mixed-Methods Evaluation: Use a mixed-methods approach to evaluate the effectiveness and impact of the pilot interventions. Quantitative methods such as surveys, health metrics analysis, and usage statistics can assess changes in healthcare access, utilisation, and outcomes. Qualitative methods such as interviews, focus groups, and case studies can provide insights into user experiences, perceptions, and contextual factors influencing intervention effectiveness.
Participatory Action Research: Engage SHG members, community leaders, and healthcare providers as active participants throughout the research process. Foster collaboration, co-design, and co-evaluation to ensure that interventions are responsive to community needs, culturally sensitive, and sustainable beyond the project duration.
Ethical Considerations: Adhere to ethical guidelines and principles throughout the research process, including informed consent, privacy protection, confidentiality, and respect for cultural values and beliefs. Ensure that interventions prioritize the well-being and autonomy of SHG members and their communities.
Dissemination and Knowledge Sharing: Share findings, lessons learned, and best practices with relevant stakeholders through workshops, conferences, policy briefs, and academic publications. Foster knowledge exchange and collaboration to promote the scale-up and replication of successful AI-driven interventions for enhancing PHC access in low-income settings and SHG contexts.
Timeline
Aug - Sept 2024: Resource setup and planning
Conduct a kickoff meeting to deliberate on research objectives, methodology, and timeline and document a detailed project plan encompassing milestones, deliverables, and budget allocation.
Undertake a literature review on AI applications in healthcare and SHG dynamics.
Extend invitations for partnerships with local organisations, SHGs, and healthcare providers.
Oct - Nov 2024: Needs Assessment and Technology Assessment
Carry out needs assessment activities such as surveys, interviews, and focus group discussions with SHG members and community stakeholders.
Analyse data collected from the needs assessment to pinpoint key healthcare challenges and priorities.
Assess Open Constitution AI network technologies for suitability in addressing identified needs.
Select appropriate AI tools based on assessment results for pilot implementation.
Dec 2024 - January 2025: Pilot Intervention Development and Preparation
Customise selected AI interventions, including telemedicine platforms & decision support systems using human augmentation.
Conduct training sessions for project volunteers & healthcare providers on using AI technologies.
Establish data collection & monitoring mechanisms to track intervention outcomes.
Obtain necessary approvals from relevant authorities for pilot implementation.
Feb - Apr 2025: Pilot Intervention Implementation
Launch pilot interventions in selected communities by deploying the AI model within the virtual private network of Open Constitution. Provide ongoing support & troubleshooting for users during implementation. Monitor intervention usage & effectiveness through data collection methods. Hold regular stakeholder meetings to review progress.
May - Jun 2025: Evaluation And Analysis
Collect quantitative & qualitative data on intervention outcomes, including changes in healthcare access & health outcomes. Analyse data using appropriate statistical methods.
Synthesise findings to assess the impact of AI interventions within communities. Identify lessons learned, success factors, areas of improvement, and model finetuning.
Jul 2025: Dissemination and Knowledge Sharing
preparing project reports, presentations, and publications summarising findings and recommendations. Additionally, organising dissemination events such as workshops, conferences, and stakeholder meetings to share project outcomes with relevant audiences is required.
Facilitating knowledge exchange and collaboration among stakeholders to promote the adoption and scale-up of successful AI-driven interventions is also part of the responsibilities. Furthermore, developing a sustainability plan for maintaining and expanding AI interventions beyond the project period, including securing funding and institutional support, is essential.
Throughout the project, maintain regular communication and collaboration among project team members, partners, and stakeholders to ensure alignment with project goals and objectives. Adjust the implementation plan as needed based on emerging insights, challenges, and opportunities encountered during project execution.
Assessment:
Expected Outcomes:
Short-Term:
Increased access to primary healthcare services among members of self-help groups (SHGs) and their families in low-income settings.
Improved utilization of AI-powered healthcare interventions, including telemedicine platforms, mobile health applications, and decision support systems.
Enhanced capacity of community health workers and SHG members to utilize AI technologies for healthcare delivery.
Positive feedback and satisfaction from SHG members, healthcare providers, and community stakeholders regarding the usability, effectiveness, and cultural appropriateness of AI interventions.
Preliminary evidence of improvements in healthcare outcomes, such as reduced morbidity, improved health-seeking behaviour, and increased adherence to preventive and treatment measures.
Long-Term:
Sustainable integration of AI-driven healthcare interventions into routine primary healthcare services within SHG communities and healthcare facilities.
Equitable improvement in health outcomes across SHG members and their families, leading to reductions in healthcare disparities and improved overall well-being.Strengthened healthcare systems and community resilience to health challenges through the adoption of innovative AI technologies and participatory approaches.
Enhanced collaboration and partnerships between local organizations, SHGs, healthcare providers, and other stakeholders to support ongoing innovation and improvement in healthcare delivery.
Potential scalability and replication of successful AI interventions to other similar settings and communities, contributing to broader efforts to achieve universal health coverage and Sustainable Development Goals related to health.
Evaluation Criteria for Success:
Increased access to healthcare: Measure the percentage of SHG members and their families accessing healthcare services before and after the intervention.
Utilization of AI interventions: Track the usage metrics of AI-powered healthcare platforms, including the number of consultations, user engagement, and frequency of use.
Capacity building: Assess the knowledge, skills, and confidence of community health workers and SHG members in utilizing AI technologies through pre- and post-training evaluations.
User satisfaction: Administer surveys and feedback mechanisms to gather user satisfaction ratings and qualitative feedback on the usability and effectiveness of AI interventions.
Health outcomes: Monitor key health indicators and outcomes, such as disease prevalence, immunization coverage, maternal and child health indicators, and changes in health-seeking behaviour over time.
Sustainability and scalability: Evaluate the sustainability of AI interventions through indicators such as ongoing usage, institutional support, funding mechanisms, and potential for replication in other settings.
By systematically tracking these short-term and long-term outcomes and evaluating them against predefined criteria for success, the project can assess its effectiveness in achieving its objectives and generating positive impacts on healthcare access and outcomes within SHG communities.
Preliminary findings for deploying a pilot AI deep learning model:
In the preliminary findings, the research group has documented and generated classified public data sets to be further used in this research:
Geolocation-mapped beneficiary profile in semi-rural, semi-urban and rural settings in India for the planned rollout or delivery of an autonomous digital public service using Gender, income and nutrition level demographics
Identification and mapping of the income levels of the beneficiary through the data reported in the SHG bank linkage programme.
Mapping of the livelihood and sustenance levels of the beneficiary population into the data set.
Geolocation mapped skill gap data set for health care practitioners for quality assurance and compliance review of the AI Service’s training set and human augmentation process
identified the livelihood settings and disease burden in these households.
Commercialisation potential:
The base model is supposedly open-source (OCL v1). The authors do not wish to patent the research outcome. The research outcome necessarily establishes standards, and these standards can be adhered to if the resultant commercialised service is deployed on the defined Open Constitution AI network.
The controls and checks have been deployed on the defined Open Constitution AI network, and its service delivery model is described in the private network’s governance model.
The network maintainer - Muellners Foundation, has established relationships with Google Cloud and AWS Cloud to scale the Sentient Bot service through the AWS Activate Program and Google Cloud Not-for-Profit program. The platform has implemented standards like HIPAA at a foundational level.
The SHG bank linkage programme can further give entry to scalable commercial aspects of the AI service.
Specific Engagement methodology with non-academic stakeholders to undertake Proof of Concept:
The research team plans to organise an operational usage of the AI service for a 1-3 month period amongst the group of network participants. The team plans to do so in cooperation with the Muellners Foundation, which onboards NPOs and medical research universities in the country, where SHGs are linked to daily wage women labourers as the target beneficiaries.